

About Lehe
乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。


乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。



So, in today's rapidly developing science, is there a method that can provide such patients with long-term and stable treatment effects? Let's take a look at Mr. Ma's treatment process and see what insights we can gain.
Overview of the illness
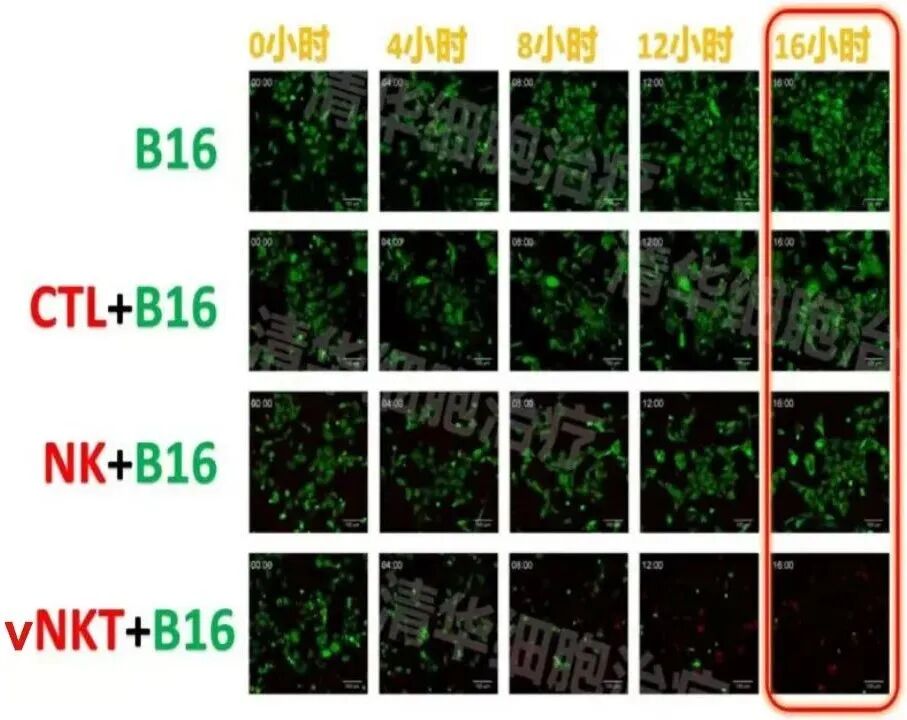
Experimental conditions: In the presence of vNKT cells, after 16 hours, nearly all B16 tumor cells were killed!
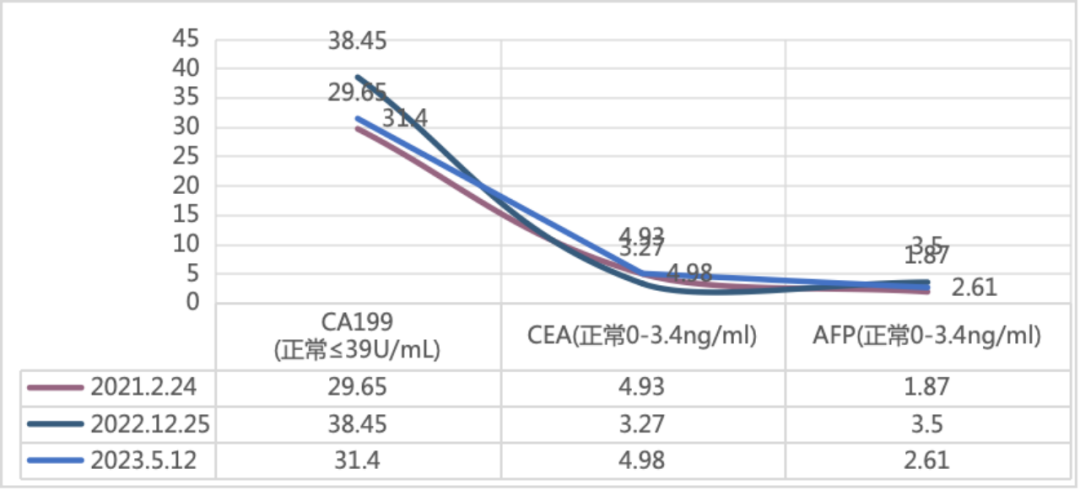
Changes in tumor markers
Imaging changes
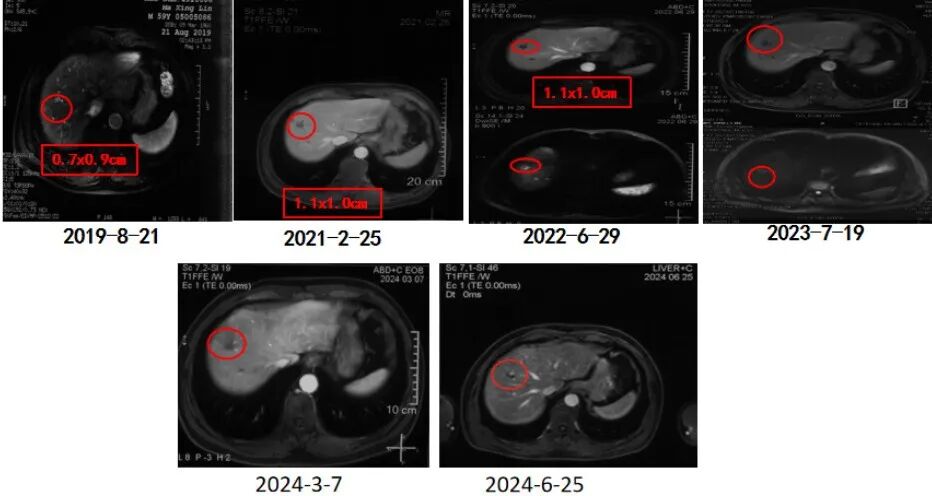
Abdominal MRI showed a nodular abnormal signal in the right anterior lobe of the liver on August 21, 2019, measuring approximately 0.7x0.9cm in size. Combined with imaging findings, liver cancer was considered a possibility. On 2252021, a follow-up MRI revealed irregular edges of the liver and a lesion cross-sectional size of approximately 1.1cmx1.0cm. Dynamic contrast-enhanced imaging with GD-EOB-DTPA injection did not show significant abnormal enhancement, consistent with MRI findings after intervention in the right anterior lobe of the liver. On 292022, a follow-up MRI showed no significant change in size compared to previous scans, but the DWI sequence showed a circular high signal shadow, indicating residual tumor activity. On 192023, a follow-up MRI showed no enhancement, indicating post-treatment changes. On March 7, 2024, a follow-up MRI showed no enhancement, indicating changes after interventional therapy. On 252024, a follow-up MRI after ablation showed no enhancement and regular follow-up is recommended.
Conclusion and Commentary

Click on the image to view past exciting content


References:
[1] CONCORD Working Group. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries[J]. Lancet, 2018; 391(10125):1023-75.
[2]MURAI H, KODAMA T, MAESAKA K, et al. Multiomics identifies the link between intratumor steatosis and the exhausted tumor immune microenvironment in hepatocellular carcinoma[J]. Hepatology, 2023, 77(1): 77-91. DOI: 10.1002/hep.32573
[3]HILL A, OLUMBA F, CHAPMAN W. Transplantation for hepatocellular carcinoma[J]. Surg Clin North Am, 2024, 104(1): 103-111. DOI: 10.1016/j.suc.2023.09.002.
[4]KARDASHIAN A, FLORMAN SS, HAYDEL B, et al. Liver transplantation outcomes in a U.S. multicenter cohort of 789 patients with hepatocellular carcinoma presenting beyond Milan criteria[J]. Hepatology, 2020, 72(6): 2014-2028. DOI: 10.1002/hep.31210.
[5]CHOI J, JO C, LIM YS. Tenofovir versus entecavir on recurrence of hepatitis B virus-related hepatocellular carcinoma after surgical resection[J]. Hepatology, 2021, 73(2): 661-673. DOI: 10.1002/hep.31289.
[6]RASIC G, de GEUS SWL, BEAULIEU-JONES B, et al. A nationwide propensity score analysis comparing ablation and resection for hepatocellular carcinoma[J]. J Surg Oncol, 2023, 127(7): 1125-1134

Address: Room 1101 (Unit 101), 11th Floor, Building 1, No. 7 Courtyard, Kexueyuan Road, Life Science Park, Changping District, Beijing
Phone:010-8265 9866
Email:lehemedneo@hotmail.com