

About Lehe
乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。


乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。

01
Case Analysis
If you cannot understand the subsequent professional description
you can finish reading this text in two minutes
Mrs. Li's condition assessment

Pancreatic cancer is highly malignant, and the pathological types of patients are complex - "moderately-poorly differentiated", "adenosquamous carcinoma", and also have "sarcomatoid" structures, which increases the risk of subsequent recurrence and metastasis.
The patient developed postoperative ascites and peritoneal effusion, which decreased after adjuvant chemotherapy but still persisted, and should not be taken lightly.
The routine follow-up after chemotherapy indicates suspicious signals in the residual pancreas and right lobe of the liver. Considering the elevated tumor marker, the possibility of disease progression in the patient has increased.
NKT cell immunotherapy can delay the time of recurrence and metastasis, and it is currently the best time for patients to undergo treatment.
In December 2019, Mrs. Li underwent NKT cell therapy. Due to her high risk of subsequent recurrence and metastasis, an intensive regimen of two courses per month was adopted for treatment.
Now, six months later, after eight consecutive courses of systematic treatment, three follow-up visits, and imaging examinations, no clear signs of tumor recurrence have been observed, and the tumor marker CEA has returned to normal levels. This indicates that the previously high risk of recurrence and metastasis has been suppressed.
02
Treatment Overview
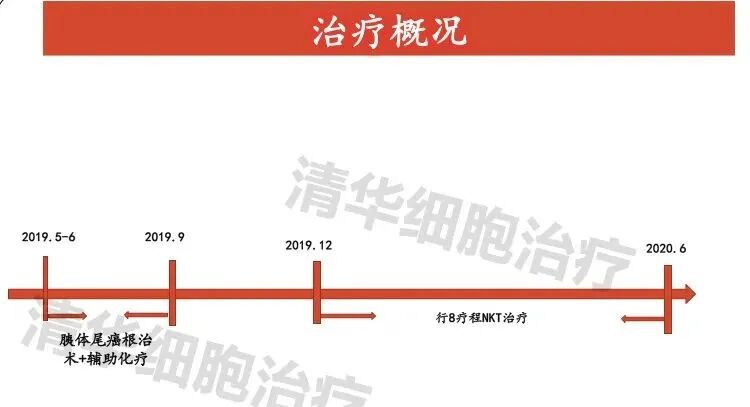
On December 12, 2018, a patient underwent an abdominal and pelvic CT scan, which revealed a low-attenuation mass shadow in the pancreatic body with a rough margin and a size of approximately 2.9*1.8cm. The possibility of pancreatic body cancer was considered, with adjacent structures being involved.
On April 9, 2019, Normal range of tumor markers: CEA 4.28ng/ml, CA19-9 <0.6U/ml.
On May 17, 2019, pathology revealed the following: 1. (Pancreas, spleen, left adrenal gland) resection specimens: (Pancreas) Combined with morphological and immunohistochemical results, the lesion was consistent with moderately-to-poorly differentiated adenosquamous carcinoma, with small foci exhibiting sarcomatoid structures and focal areas accompanied by significant fibrosis. No definite intravascular thrombi or neural invasion was observed. No cancer was detected at the pancreatic resection margin, no definite metastasis was found in the lymph nodes surrounding the pancreas, and no definite cancer involvement was observed in the spleen and adrenal glands. 2. (Hepatic artery nerve plexus resection margin) was examined and found to consist of fibrous adipose connective tissue and nerve fiber bundles, with no cancer detected. 3. (Celiac artery mesenteric nerve plexus) was examined and found to consist of fibrous adipose connective tissue and nerve fiber bundles, with no cancer observed.
From June 25, 2019 to September 24, 2019, received adjuvant chemotherapy with a 4-cycle regimen of gemcitabine plus temozolomide.
On June 18, 2019, abdominal CT reexamination showed: after resection of the pancreatic body and tail, spleen, and left adrenal gland; the fluid accumulation in the abdominal and pelvic cavity decreased compared to before.
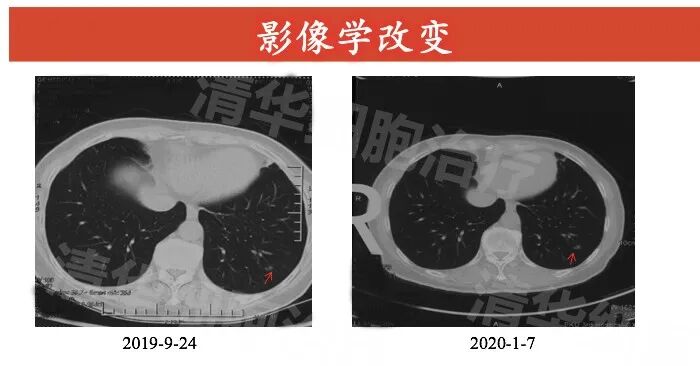
On September 25, 2019 CT showed: 1. A few fibrous streaks in both lungs 2. Small nodules in the lower lobe of the left lung.
On September 26, 2019, an MR plain scan of the upper abdomen showed: changes after resection of the pancreatic body and tail and spleen, as well as the left adrenal gland; suspicious abnormal signals in the residual pancreatic parenchyma, with no abnormal high signals on DWI; the abnormal signal in the right lobe of the original liver was similar to that observed previously (June 19, 2019).
On December 10, 2019, began NKT cell immunotherapy, with a regimen of 2 courses per month. So far, 8 courses have been completed (as of the imaging review time in June 2020).
03
Imaging data
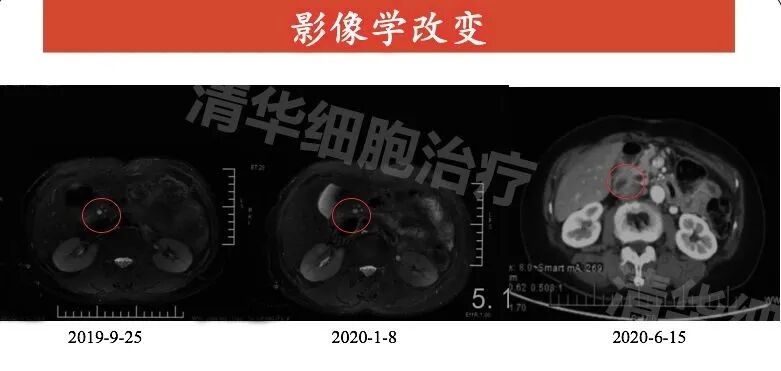
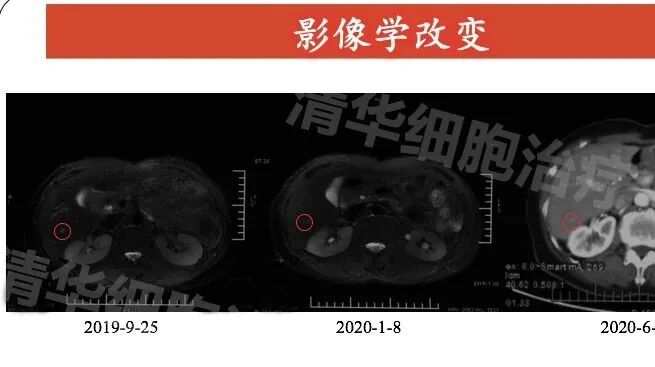 Abdominal MR: pancreatic body and tail, spleen, left adrenal gland resection postoperative changes, patchy slightly long T2 signal intensity visible in the right lobe of the liver, with no significant size change from September 2019 to January 2020.
Abdominal MR: pancreatic body and tail, spleen, left adrenal gland resection postoperative changes, patchy slightly long T2 signal intensity visible in the right lobe of the liver, with no significant size change from September 2019 to January 2020.
Abdominal CT: Compared to September 2019 and January 2020, there was no significant change in size in June 2020.


04
Tumor markers

NKT Classic Case Review
Click on the image
to view
 THE END
THE END 
Address: Room 1101 (Unit 101), 11th Floor, Building 1, No. 7 Courtyard, Kexueyuan Road, Life Science Park, Changping District, Beijing
Phone:010-8265 9866
Email:lehemedneo@hotmail.com