

About Lehe
乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。


乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。


▲Click the blue text to follow us
"Blood in stool, diarrhea, abdominal pain" - these symptoms should never be ignored. You may think they are just occasional diarrhea, but they could be early signs of rectal cancer. Rectal cancer, as a type of colorectal cancer, often presents with subtle early symptoms, leading many patients to be diagnosed with advanced disease.
The latest data on the burden of malignant tumors in China, released by the National Cancer Center (NCC) in February 2024, shows that an estimated 4.8247 million new cases of malignant tumors occurred nationwide in 2022, with lung cancer ranking first in incidence among malignant tumors. Among them, colorectal cancer (517,100 cases, accounting for 10.7%) ranked second. [1] Colorectal cancer, also known as large intestine cancer, generally includes rectal cancer and colon cancer. The rectum, a segment of the terminal end of the intestinal tract, is approximately 12-15 centimeters long and is a high-risk area for cancer development in all intestinal tracts.
Disease Overview
Ms. Zhang visited the hospital in February 2020 due to increased frequency of bowel movements and blood in her stool.
► Colonoscopy: At the junction of the rectum and the sigmoid colon, approximately 18cm into the scope, an ulcerative infiltrative lesion was visible, with obvious surface erosion, irregular raised edges, easy bleeding upon contact, slightly narrowed lumen, and a tough biopsy texture.
► Pathology: High-grade intraepithelial neoplasia with carcinogenesis in the mucosal gland epithelium.
On February 27, 2020, a radical resection of rectal cancer was performed.
►Postoperative pathology: 1. (Rectal) adenocarcinoma, grade II, ulcerative type, approximately 3.1cm x 2.5cm x 1cm in size, with cancer tissue invading the subserosal fat tissue, and visible vascular invasion. 2. No cancer tissue involvement was observed in both rings of the (anastomotic stoma) upon examination. 3. Mesenteric lymph nodes (+), 8/22 nodes. 4. AJCC PTNM staging (8th Ed, 2017): PT4N2. 5. Immunohistochemical results: PMS2 (+), MSH2 (+), MSIH6 (+), MLH1 (+). Postoperative chemotherapy for 12 cycles.
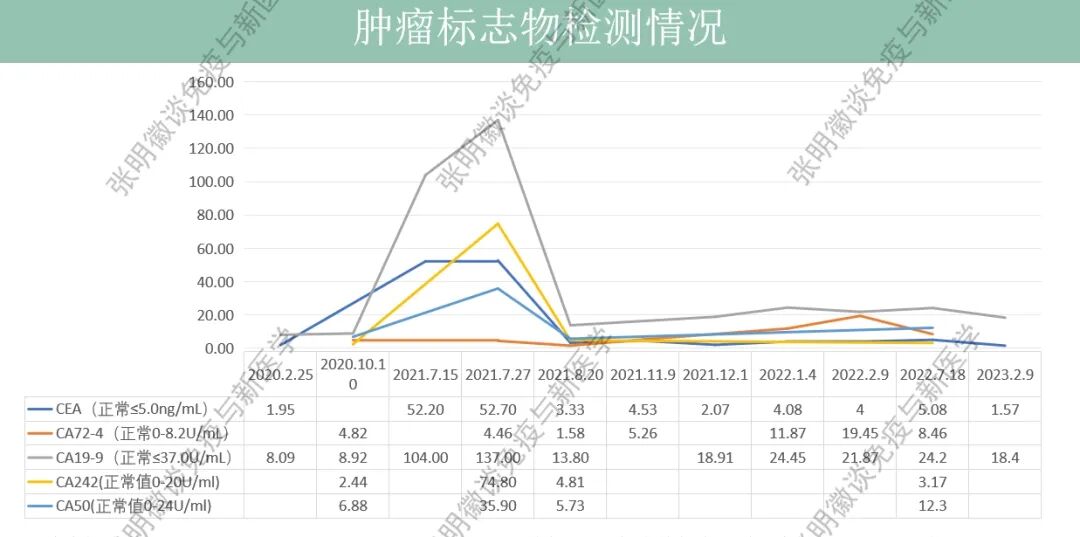
►On July 15, 2021, tumor markers: CEA and CA19-9 increased. MR: Compared with the film on April 19, 2021: mass in the left lobe IV segment of the liver, unclear boundary, edge enhancement, approximately 38*22mm, possible metastasis. On July 28, 2021, surgical treatment was performed on the liver metastasis foci, followed by postoperative chemotherapy with temozolomide.
Tips
Staging and Grading of Rectal Cancer
● The commonly used staging system for rectal cancer is TNM staging, with stages I, II, III, and IV.
● Clinical TNM staging is mainly based on the number of regional lymph node metastases, the extent of the primary lesion, and whether there is distant metastasis.
● T indicates the extent of the primary lesion of rectal cancer, clinically divided into T0 (no rectal cancer lesion), Tis (carcinoma in situ), T1 (involvement of the submucosal layer), T2 (involvement of the muscular layer), T3 (involvement of the adventitia), and T4 (involvement of the perirectal tissue).
N represents the status of regional lymph node metastasis. It is divided into N0 (no lymph node metastasis), N1 (1-3 lymph node metastases), and N2 (more than 4 lymph node metastases) based on the number of lymph node metastases.
M indicates whether the tumor has distant metastasis, with M0 (no distant metastasis) and M1 (distant metastasis).
● According to different degrees of infiltration, staging can be divided into Stage I, where the tumor is limited to the mucosa and submucosa without lymph node metastasis. Stage II involves tumor invasion of the muscularis propria without lymph node metastasis. Stage III involves tumor invasion of the subserosa or perirectal tissue, with lymph node metastasis. Stage IV involves distant organ metastasis, commonly to the liver, bones, and lungs.
Stage III is a watershed, be cautious of recurrence and metastasis
Professor Zhang Minghui, an immunology expert from Tsinghua University, interprets the characteristics of Stage III tumors
Ms. Zhang was diagnosed with rectal cancer in February 2020, and postoperative pathology showed PT4N2, which belongs to Stage III tumor.
Tumor staging is one of the most important factors affecting prognosis . Stage III is a watershed, and it is a stage prone to recurrence and metastasis. Stage III rectal cancer refers to the condition where the cancer has invaded the serosal layer of the rectum or surrounding tissues, with lymph node metastasis, and is classified as mid-to-late stage rectal cancer. The treatment is challenging, and the prognosis is relatively poor. If the patient is elderly, in poor physical condition, or has other comorbidities, it may increase the difficulty and risk of treatment.
In July 2021, Ms. Zhang underwent surgical treatment for liver metastasis foci. Within just over a year, Ms. Zhang's condition recurred and metastasized, progressing to Stage IV. Stage IV rectal cancer is characterized by distant metastasis, with a relatively poor prognosis, necessitating a comprehensive treatment strategy.
vNKT cell immunotherapy breaks the survival dilemma of advanced bowel cancer
After understanding the characteristics of advanced rectal cancer, Ms. Zhang promptly contacted Professor Zhang Minghui's team at Lehe New Medicine to discuss vNKT cell therapy.
Tips
vNKT Cell Therapy
The vNKT immune cell subpopulation discovered by Zhang Minghui's team at Tsinghua Universitypossesses both the non-specific recognition function of NK cells and the specific recognition function of CD8+T cells,thus exhibiting a dual anti-tumor effect that can rapidly kill tumor cells. It not only directly kills cancer cells but also kills inhibitory immune cells (Myeloid-derived suppressor cells, MDSCs are a heterogeneous group of cells derived from the bone marrow, capable of significantly inhibiting immune cell responses and negatively regulating immune responses.), regulating the microenvironment within cancer tissues, providing new hope for the treatment of solid tumors. Additionally, vNKT cells are collected from the immune cells of healthy individuals, cultured and expanded, and then infused back into patients, making it easier to implement the treatment.
After comprehensively understanding Ms. Zhang's condition, the Lehe New Medical team provided a second diagnosis and treatment suggestion based on a comprehensive evaluation:
1. Ms. Zhang underwent radical resection for rectal cancer, and the postoperative pathology revealed risk factors such as vascular tumor thrombus and lymph node metastasis. The risk of postoperative recurrence was high, and adjuvant chemotherapy was administered to control the disease progression as much as possible.
2. Despite undergoing 12 cycles of postoperative chemotherapy, Ms. Zhang still developed liver metastasis, indicating a high malignancy of the cancer cells.
3. After surgery and chemotherapy, the tumor burden was reduced to some extent, but there was still a risk of progression. It was recommended to undergo vNKT cell therapy to enhance the body's immunity and control tumor progression.
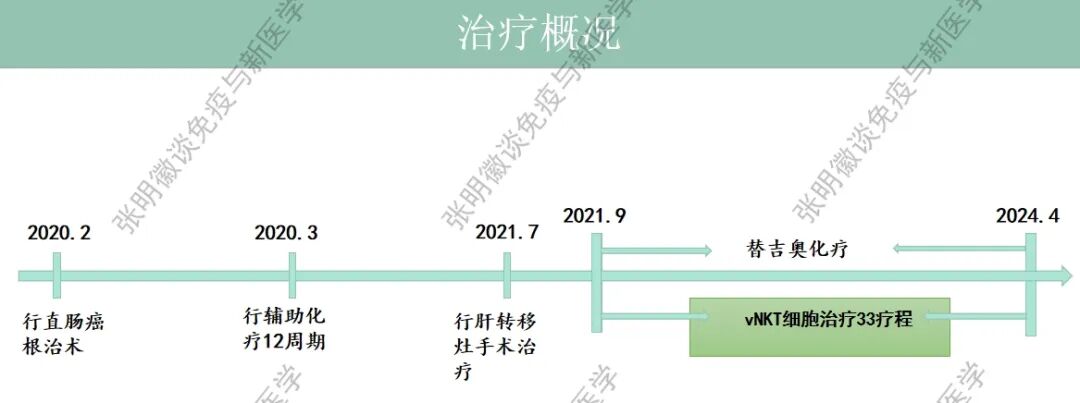
According to the second diagnosis and treatment recommendation, Ms. Zhang began vNKT cell therapy on September 23, 2021, with a treatment regimen of 2 courses per month. During the treatment, Ms. Zhang's condition remained stable, and multiple follow-up examinations showed that the lesion remained stable. Therefore, in January 2022, the treatment was adjusted to 1 course per month, and 33 courses have been completed to date (as of April 19, 2024).
Imaging changes
Pelvic imaging: Pelvic MRI in December 2021 showed postoperative changes of rectal cancer without obvious signs of recurrence or metastasis. Follow-up MRI from February 2022 to April 2024 showed no changes compared to the previous one.

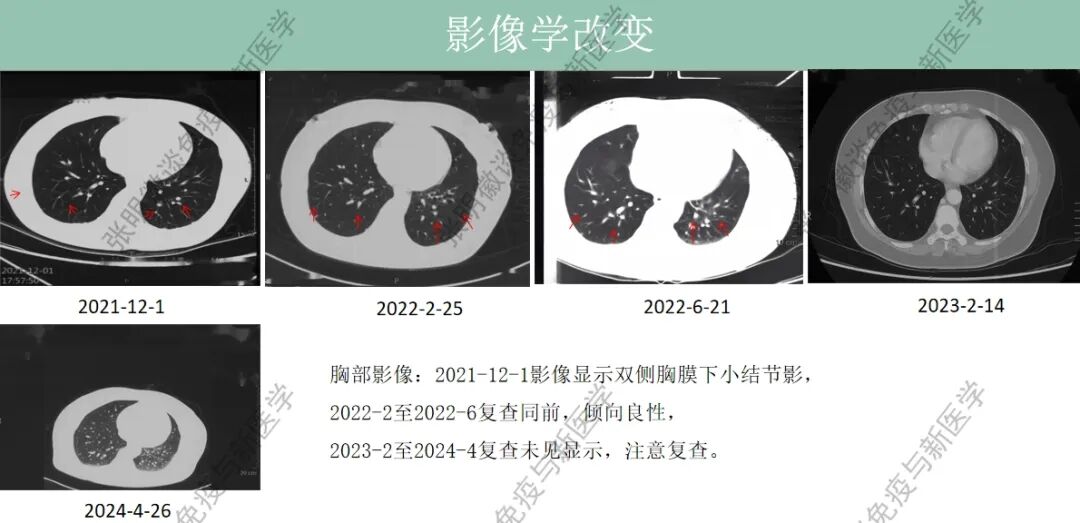
Chest imaging: Chest imaging on December 1, 2021 showed bilateral subpleural nodules, which were benign-like on follow-up imaging from February 2022 to June 2022. Follow-up imaging from February 2023 to April 2024 showed no signs of recurrence, but regular follow-up is recommended.
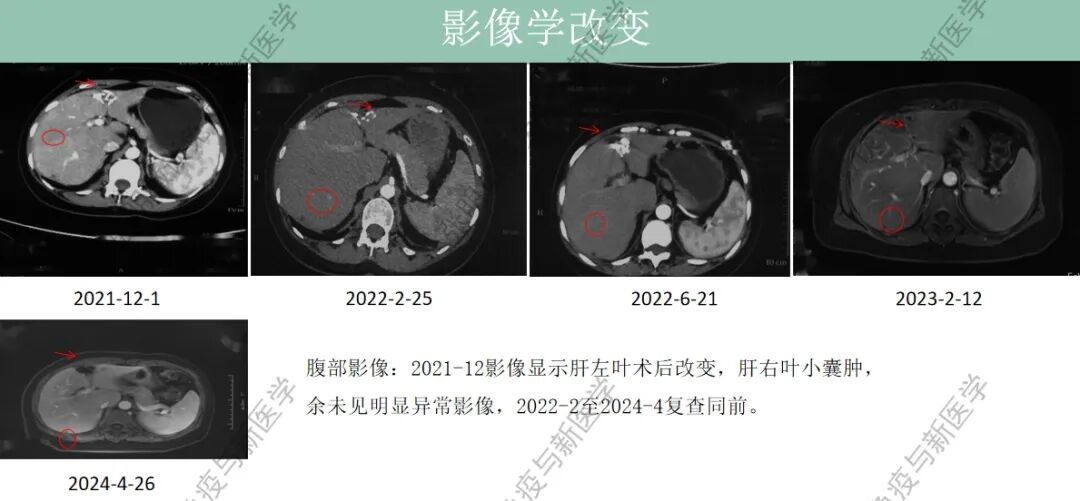
Abdominal imaging: The imaging in December 2021 showed postoperative changes in the left lobe of the liver, a small cyst in the right lobe of the liver, and no other significant abnormalities. Follow-up imaging from February 2022 to April 2024 showed no changes compared to the previous imaging.
Tumor markers: In July 2021, CEA, CA199, CA242, and CA50 were significantly elevated, but all returned to normal ranges upon follow-up in August. During the cell therapy period, CEA, CA19-9, CA242, and CA50 were all within normal ranges. From January 2022 to July 2022, CA72-4 showed intermittent elevation compared to the previous level (November 2021), and continued monitoring is required.
After vNKT cell therapy, Ms. Zhang's condition improved significantly. Her imaging follow-up results showed no abnormal signals. Ms. Zhang felt more energetic than before, and was able to carry out physical labor, such as moving heavy shopping bags or luggage (over 5kg, such as a 5-liter barrel of cooking oil), for 8 minutes (approximately 800 meters), with good sleep quality. She had no issues with normal daily life and work.
Summary
The early detection and treatment of cancer are crucial. Regular physical examinations and paying attention to abnormal bodily signals can aid in early diagnosis. For patients in the middle and late stages, postoperative preventive treatment and active treatment after recurrence and metastasis are equally important. In the early stage, Ms. Zhang underwent radical surgery to remove the primary lesion, but she still experienced recurrence and metastasis shortly thereafter. Later, even when the tumor progressed to stage IV, Ms. Zhang effectively controlled her condition and improved her quality of life through the active use of vNKT cell immunotherapy, breaking the survival dilemma of advanced intestinal cancer!
Reference source:
[1] Zheng RS, Chen R, Han BF, Wang SM, Li L, Sun KX, Zeng HM, Wei WW, He J. [Cancer Incidence and Mortality in China, 2022]. Chinese Journal of Cancer. March 23, 2024; 46(3):221-231. doi:10.3760/cma.j.cn112152-20240119-00035. PMID: 38468501.

Contact Us
Scan QR Code
Communicate with Professor Zhang Minghui's Team
Click on the Image to View Previous Highlights

Written by: Liu Fengmei
Reviewed by: Qiao Jiacheng, Wang Ying, Gao Chen
Edited/typeset by: Liu Fengmei

Address: Room 1101 (Unit 101), 11th Floor, Building 1, No. 7 Courtyard, Kexueyuan Road, Life Science Park, Changping District, Beijing
Phone:010-8265 9866
Email:lehemedneo@hotmail.com